Navigating the EU Clinical Trials Regulation (CTR): A Practical Guide for Researchers
For many non-legal professionals in European clinical research, the end of the transition period for the new EU Clinical Trials Regulation (CTR) has been a source of significant anxiety. However, the surprising truth is that the post-transition era is actually much simpler because the legal ambiguity of harmonizing old and new rules has been removed.
If you are an investigator worried about navigating a highly technical 10-year regulatory framework, here is a relieving fact right up front: unless you are the official trial “sponsor,” you do not even have to use the centralized clinical trials IT system yourself.
"I sensed that there was a bit of fear or apprehension, but in reality, it's much easier... now after the end of the transition period, it's simpler in a way just because you can rely only on the clinical trial regulation."
Here is how you can translate this complex regulation into a practical operational workflow for your daily clinical research.
The Core Shift: Why the EU Needed a Unified Clinical Trials Regulation
Historically, European clinical trials were governed by a directive, which meant member states had a wide margin of discretion on how to implement the rules. This led to a fragmented system that made transnational research incredibly difficult to coordinate.
The new CTR is designed to provide a “single entry point” that fosters unified, multinational research while giving researchers more predictable rules to operate under. Above all else, the regulation is grounded in a foundational ethical mandate:
"The general principle states that the clinical trial may be conducted only if the rights, safety, dignity and especially well-being of subjects are protected and must prevail over all other interests, economics and academics as well."
How to Streamline Multinational Trial Authorizations
Adopting the “Single Entry Point” Strategy
To launch a clinical trial across multiple EU borders, you no longer need to navigate fragmented, state-by-state approval processes. Instead, your multinational consortium must designate a single country as the “Reporting Member State” (RMS).
The sponsor submits one unified application dossier to the RMS. If the RMS authorizes the trial, that decision is generally accepted by all the other “concerned member states” participating in your research.
Navigating Part 1 and Part 2 Assessments
Once submitted, the RMS will evaluate your trial on two parallel tracks:
Part 1 Assessment: Focuses on the clinical risks, potential patient benefits, labeling, and—crucially for pediatric trials—the official opinion of the EMA’s pediatric committee.
Part 2 Assessment: An interdisciplinary review focusing heavily on the safeguards established for taking informed consent and ensuring compliance with data privacy regulations.
Patient consent: Avoiding the Most Common Legal Trap
One of the biggest pitfalls researchers encounter is confusing clinical trial consent with data privacy consent. Merging these concepts into a single form is a legal mistake; they are functionally and bureaucratically separate.
Implementing the “Two-Document” Framework
To legally safeguard your trial, you must implement a strict two-document process:
The Informed Consent Document: A clear, plain-language document detailing the medical risks, clinical benefits, trial objectives, and the patient’s right to withdraw at any time.
The Privacy Policy (GDPR Consent): A separate document explicitly asking the patient to authorize the processing of their personal and health data. If you plan to use this data for future publications or further research, it must be explicitly stated and agreed upon in this document.
"The informed consent document serves the purpose of informing the subject that they are about to start a clinical trial with some risks and with some possible benefits. Whereas it remains separate also from a bureaucratic point of view. You have two different documents... the privacy policy... through which we ask to process the personal data."
A Quick Note on Reading the CTR Text
When reviewing the actual CTR text, you might notice the GDPR is missing. Because the CTR was approved slightly before the GDPR in 2016, the text references an older data protection directive. You must mentally substitute references to that older directive with the “GDPR” when interpreting the rules.
Special Ethical Safeguards for Pediatric Clinical Trials
When running a trial involving minors, the CTR demands strict specialized oversight. Any reporting member state assessing your trial must have assessors with proven pediatric expertise.
Assessing Mental Maturity and Handling Withdrawal
In pediatric trials, informed consent is legally provided by the child’s designated legal representative (usually a parent or tutor). However, researchers are legally obligated to actively assess the mental maturity of the minor and include them in the process.
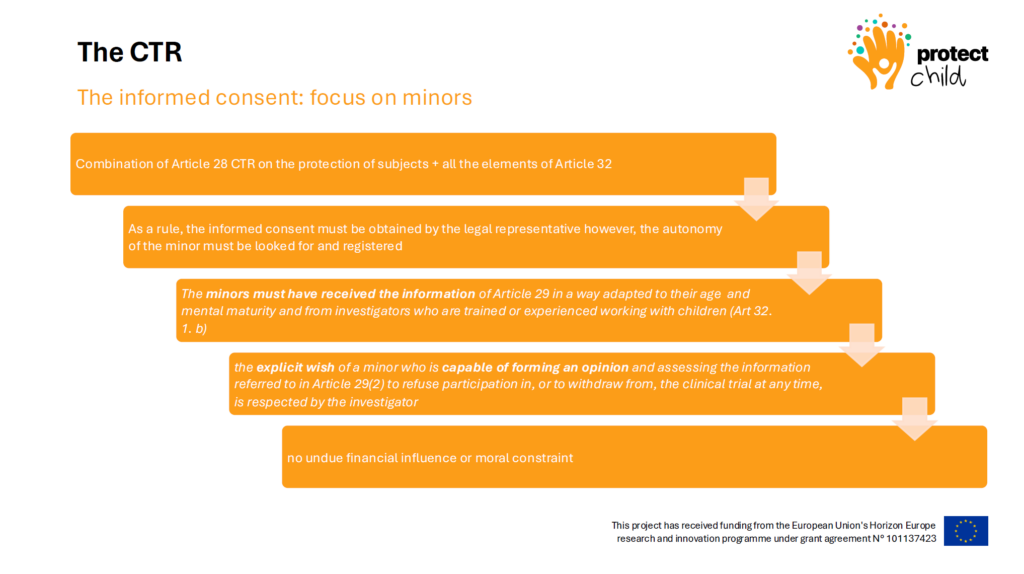
If you are dealing with an older, mature minor (e.g., a 16-year-old) who explicitly wishes to withdraw from the trial, their autonomous choice must be respected, even if the legal representative disagrees.
"The autonomy of the minor must be looked after and registered... if we have an older child that is very mature for their age, it is important to make them part of this process and also to respect the explicit wish of a minor who is capable of forming an opinion."
Building Data Infrastructures? When the MDR Does (and Doesn't) Apply
For technology partners and researchers building federated health data platforms, intersecting regulations can cause major operational roadblocks. Many mistakenly assume that because they are building health tech, the Medical Device Regulation (MDR) applies.
Applying the “Function-First” Framework
If your platform is purely an infrastructure to collect and analyze federated data for research—and does not make direct clinical decisions—the MDR does not apply to your platform.
Instead of burning resources on MDR compliance, data infrastructure projects should pivot their focus to:
GDPR Compliance: Conducting Data Protection Impact Assessments.
The European Health Data Space: Preparing for incoming centralized data-sharing rules.
Cyber-resilience Acts: Applying harmonized cybersecurity frameworks for non-medical devices.
The MDR will only trigger later if the researchers use the resulting data from your platform to manufacture a brand-new medical device.
Conclusion & Next Steps
Navigating the CTR doesn’t have to be a bureaucratic nightmare. By adopting the Single Entry Point strategy, clearly dividing your paperwork with the Two-Document Consent framework, and accurately identifying your regulatory burden with a Function-First MDR assessment, you can remove bottlenecks and focus on what matters most: conducting robust, safe, and ethical transnational research.